Optic II
| Description | Labelled | Unlabelled |
|---|---|---|
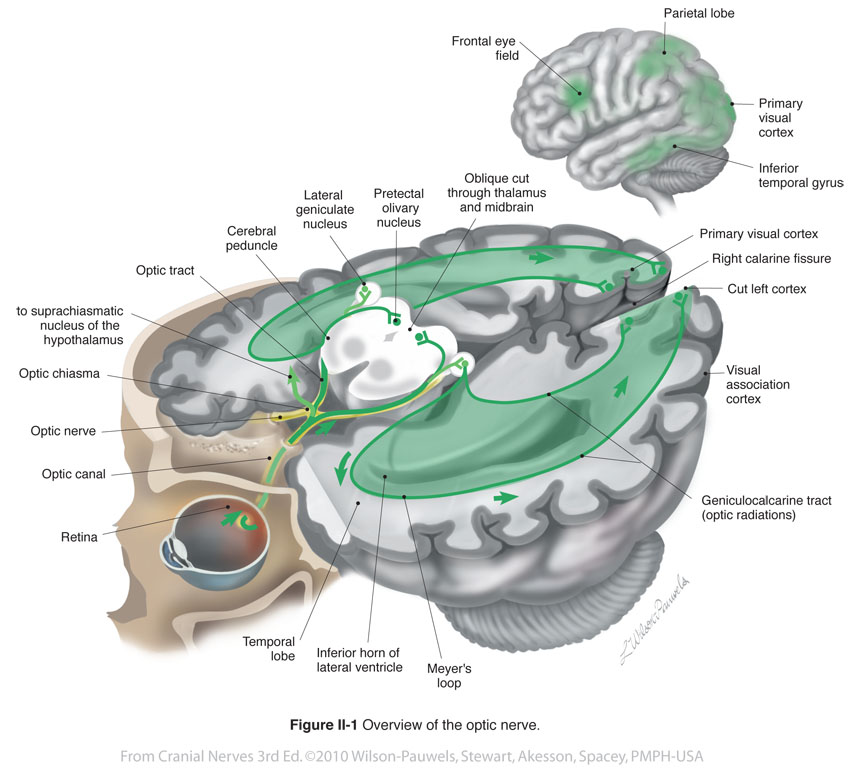
| Figure II-1 Overview of the Optic Nerve. Special sensory afferent (green) |
 |
 |
| Figure II-2 Projection of the visual field onto the retina in each eye. | 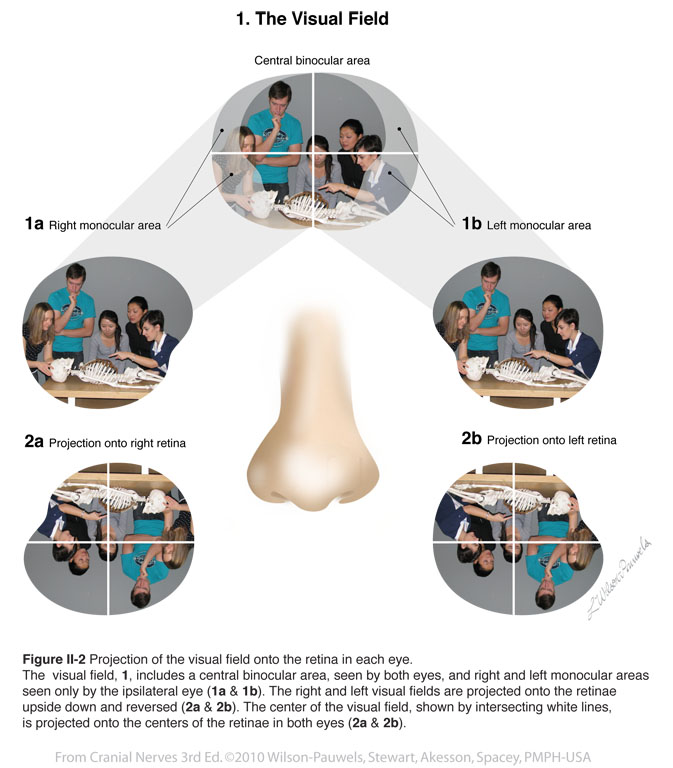 |
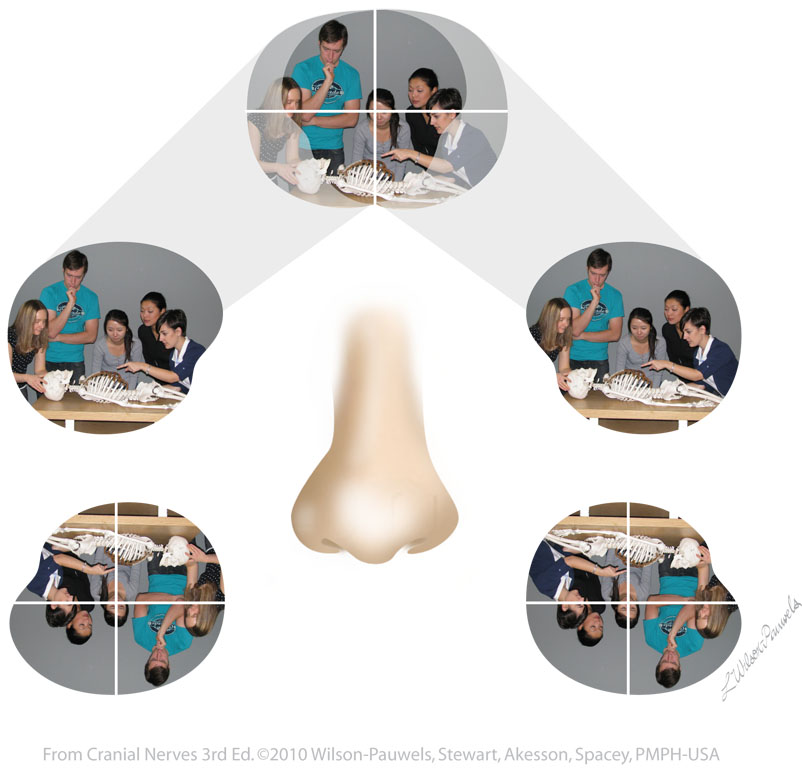 |
| Figure II-3 Due to the refraction of light through a convex lens, the visual field is projected onto the retina upside down and laterally reversed |  |
 |
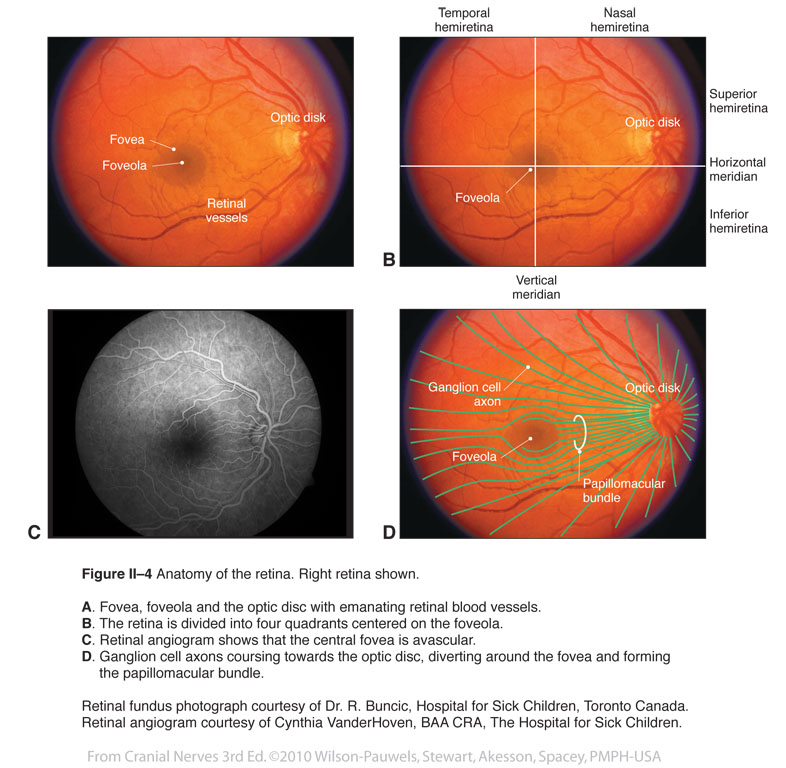
| Figure II-4 Anatomy of the retina. Right retina shown. Special sensory afferent (green) |
 |
 |
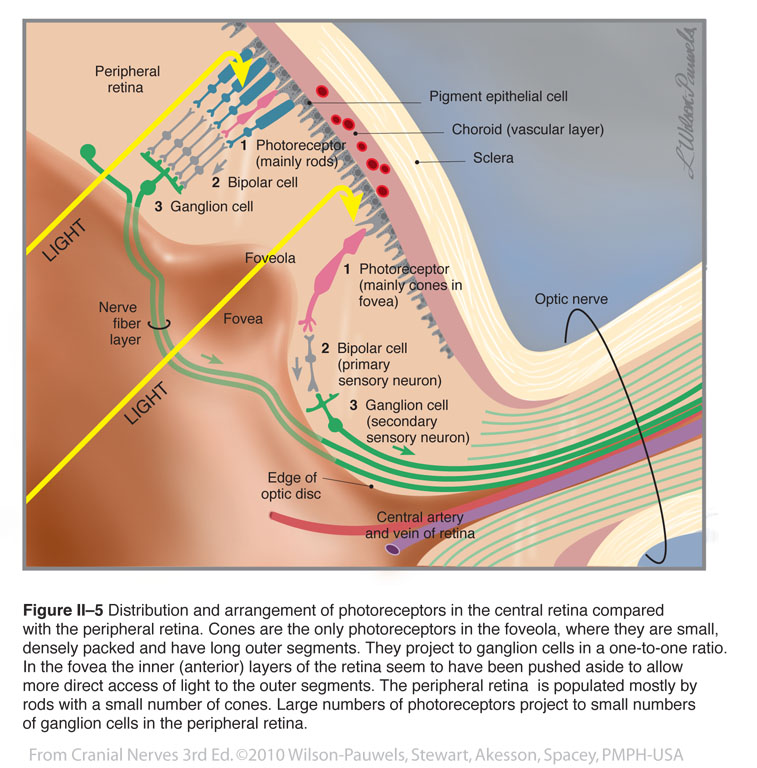
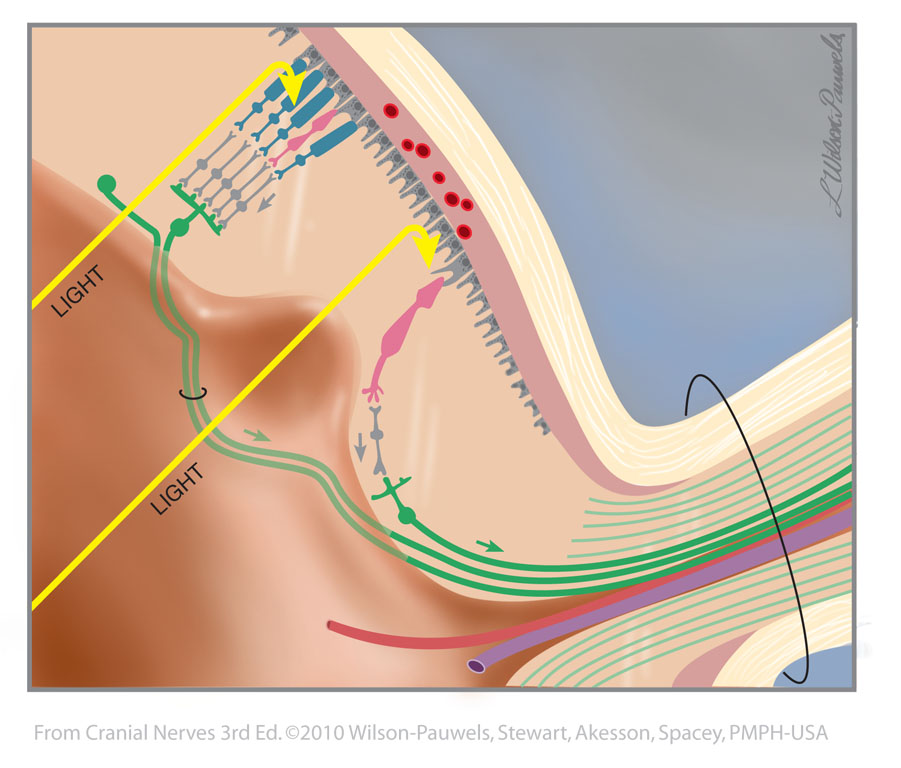
| Figure II-5 Distribution and arrangement of photoreceptors in the central and peripheral retina compared with the peripheral retina. Special sensory afferent (green) |
 |
 |
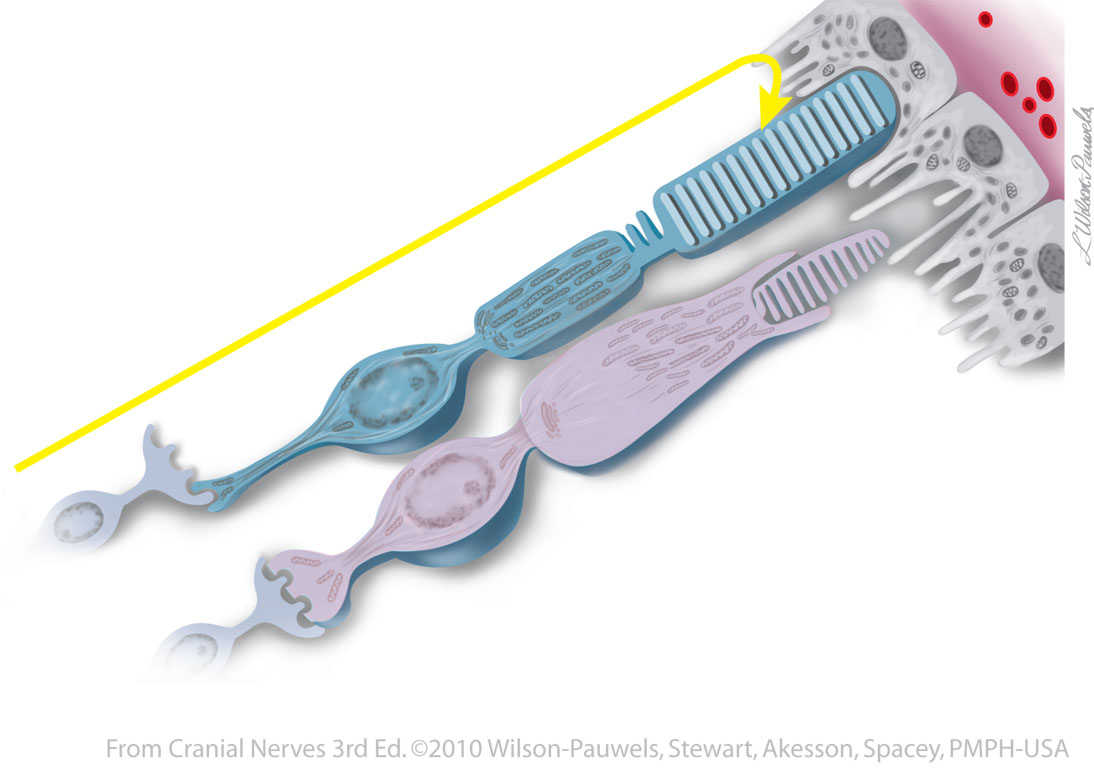
| Figure II-6 Rods and cones of the retina. | 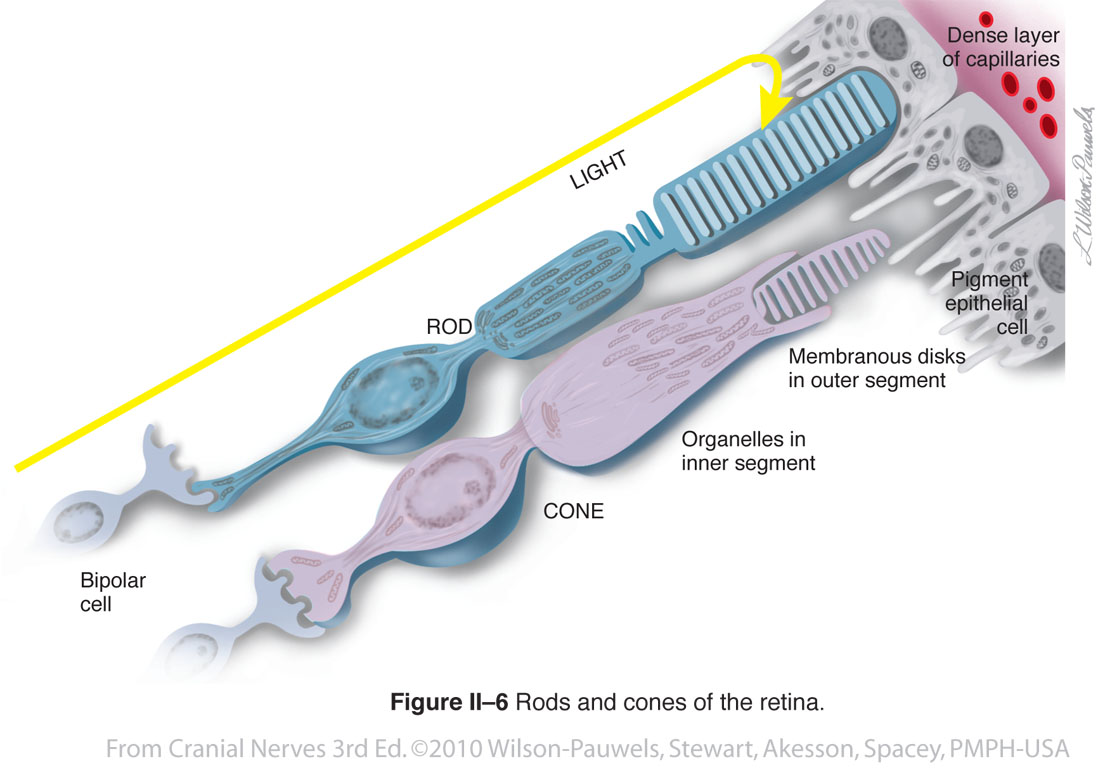 |
 |
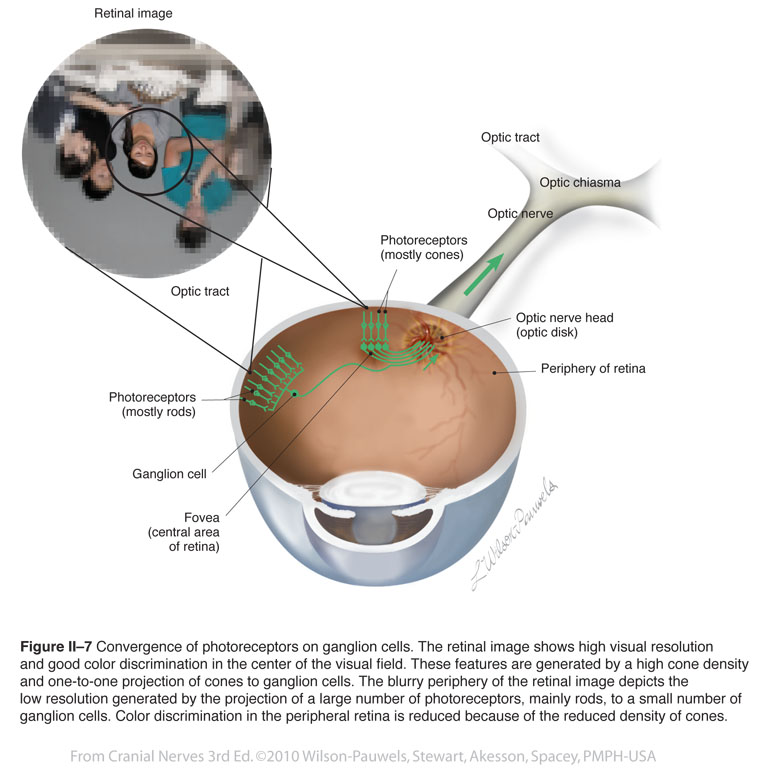
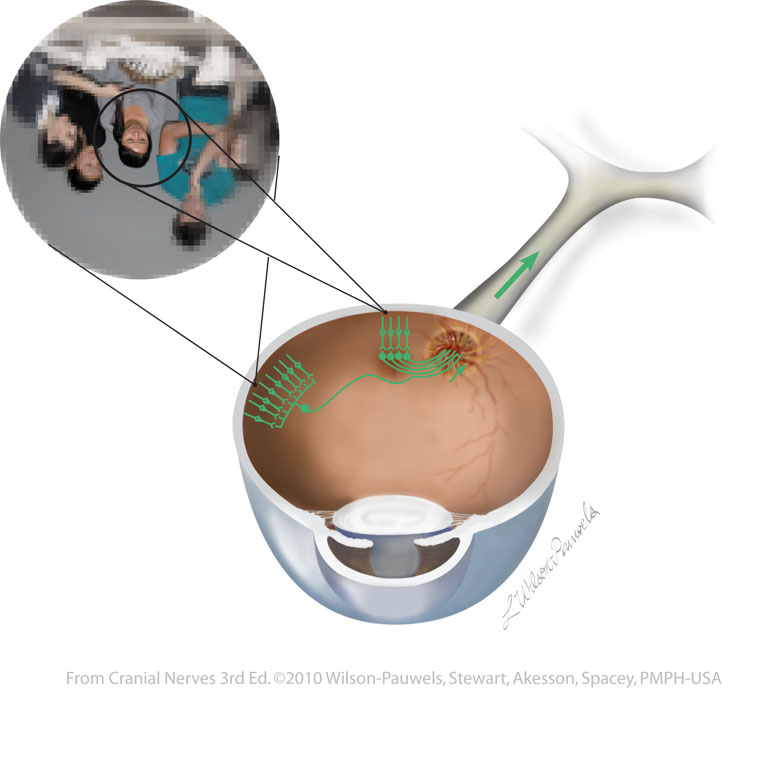
| Figure II-7 Convergence of photoreceptors on ganglion cells. Special sensory afferent (green) |
 |
 |
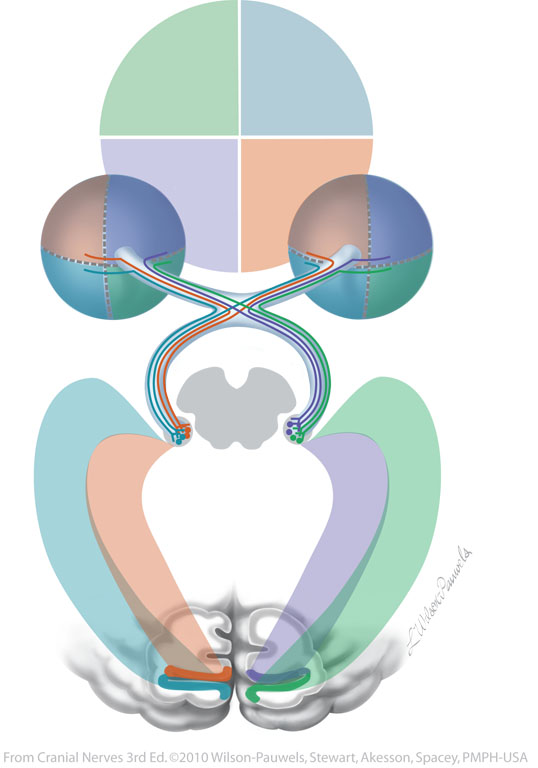
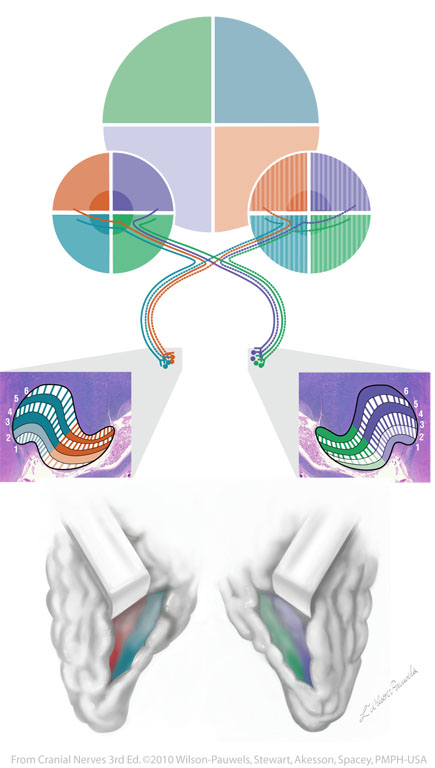
| Figure II–8 The visual pathway. The quadrants of the visual fields are color-coded to show transmission of information to the retinae and to the primary visual cortices where the image is first perceived. (Representation of the foveas are not shown in this illustration, see Figure II-9.) . |  |
 |
| Figure II–9 The primary visual cortices surrounding the calcarine fissures receive signals from the four quadrants of the visual fields via the lateral geniculate nuclei. The upper visual fields are mapped below the calcarine fissures and the lower visual fields are mapped above the calcarine fissures. |  |
 |
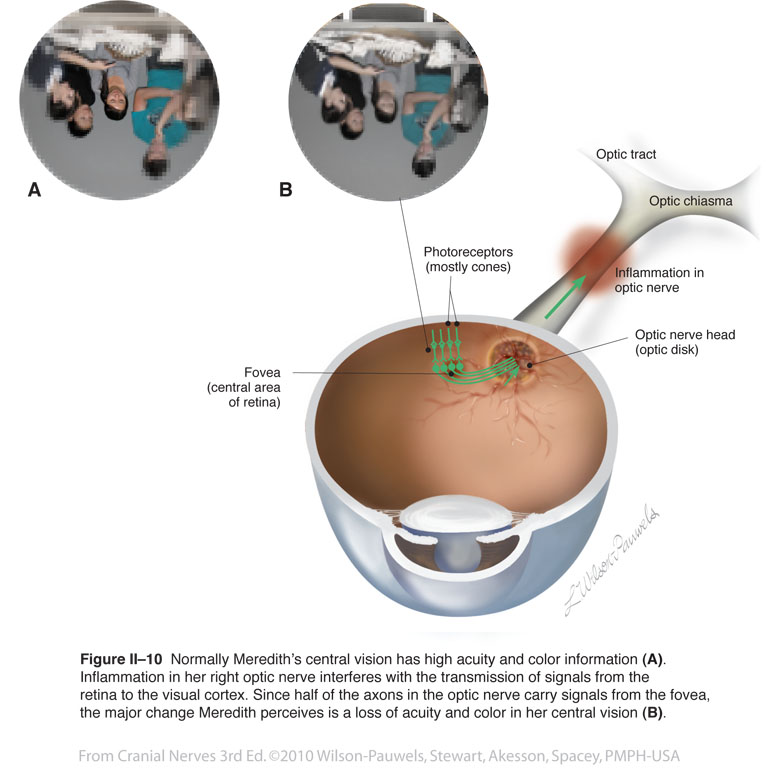
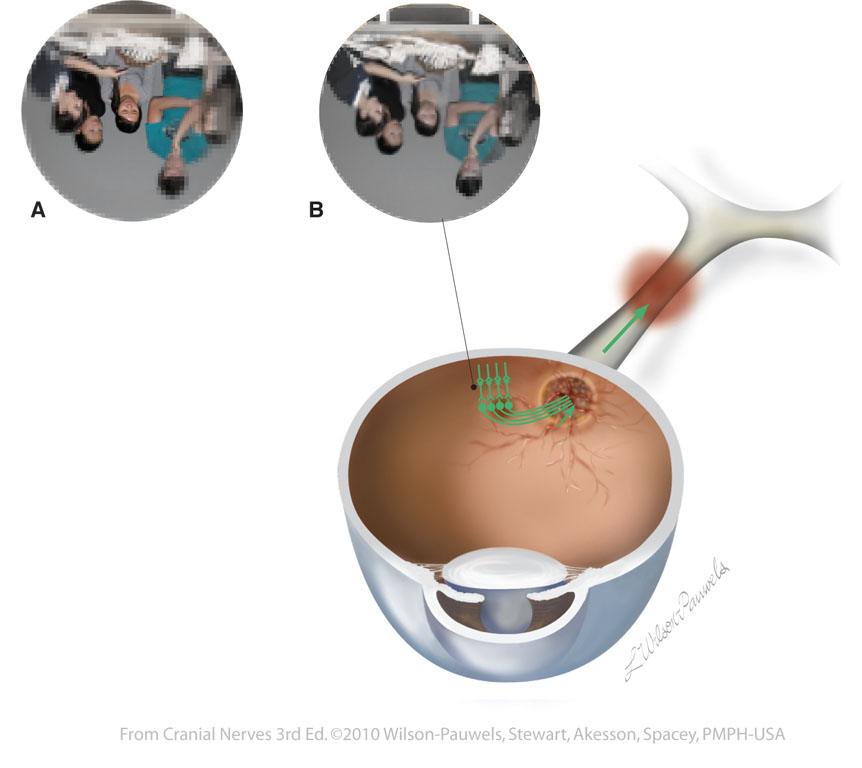
| Figure II–10 Normally Meredith’s central vision has high acuity and color information (A). Inflammation in her right optic nerve interferes with the transmission of signals from the retina to the visual cortex. Since half of the axons in the optic nerve carry signals from the fovea,the major change Meredith perceives is a loss of acuity and color in her central vision (B). Special sensory afferent (green) |
 |
 |
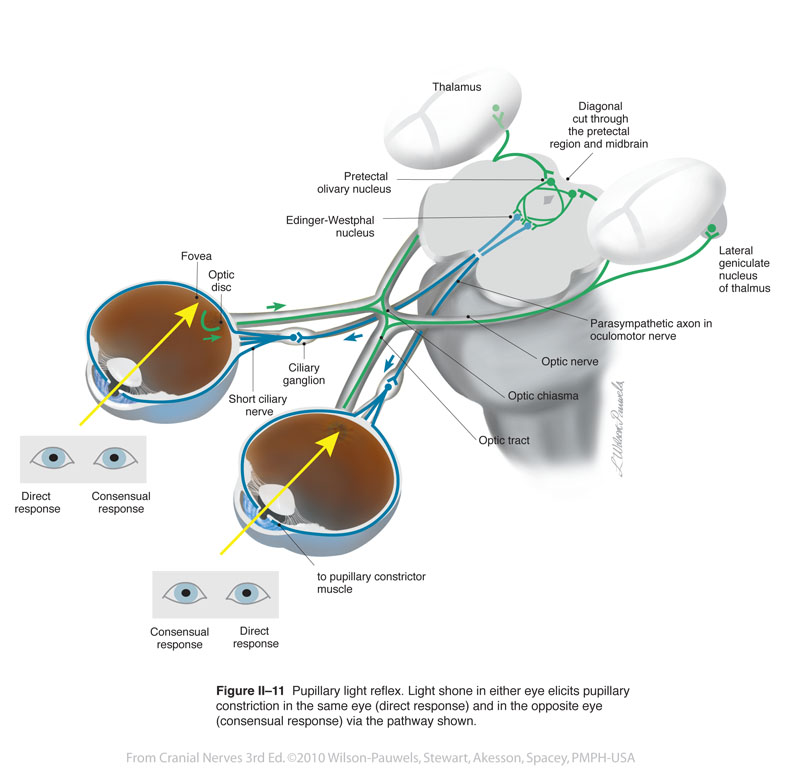
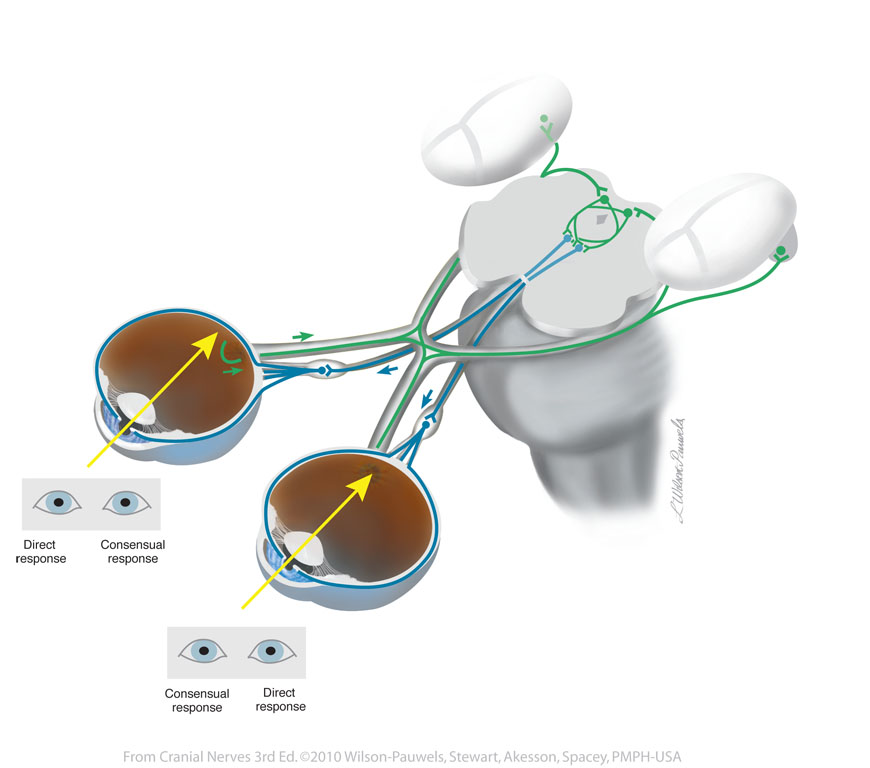
| Figure II–11 Pupillary light reflex. Light shone in either eye elicits pupillary constriction in the same eye (direct response) and in the opposite eye (consensual response) via the pathway shown. Special sensory afferent (green) Visceral motor (parasympathetic) efferent (blue) |
 |
 |
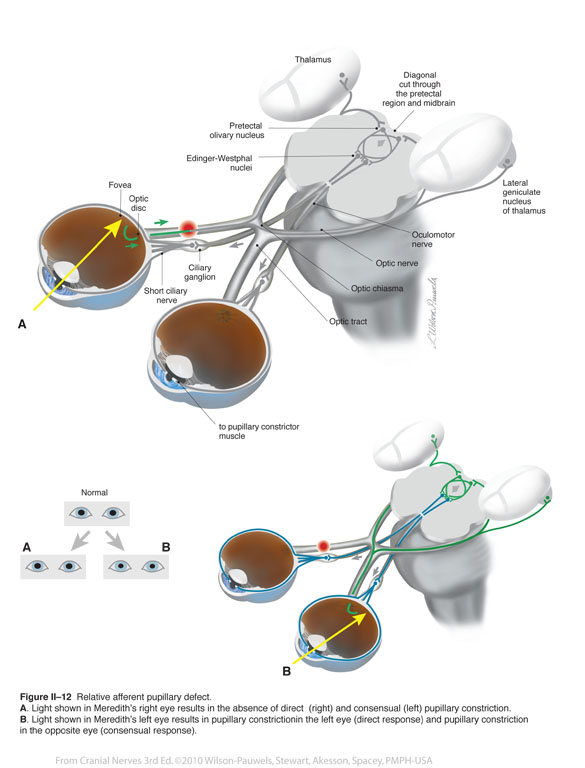
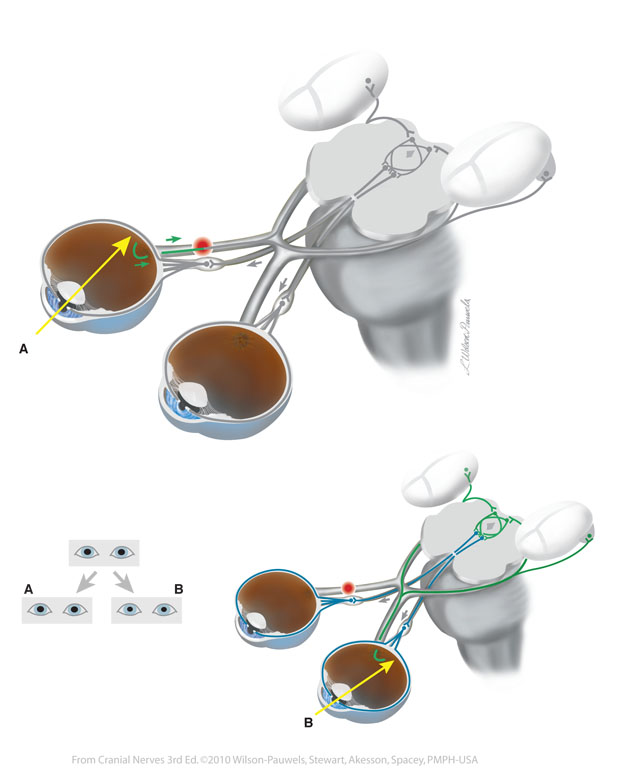
| Figure II–12 Relative afferent pupillary defect. A. Light shown in Meredith’s right eye results in the absence of direct (right) and consensual (left) pupillary constriction. B. Light shown in Meredith’s left eye results in pupillary constrictionin the left eye (direct response) and pupillary constriction in the opposite eye (consensual response). Special sensory afferent (green) Visceral motor (parasympathetic) efferent (blue) |
 |
 |
| Figure II–13 Monocular visual loss. Damage to the visual pathway anterior to the chiasm results in visual loss in the affected eye only. Damage to the left optic nerve, as illustrated, results in a loss of vision in the left eye. | 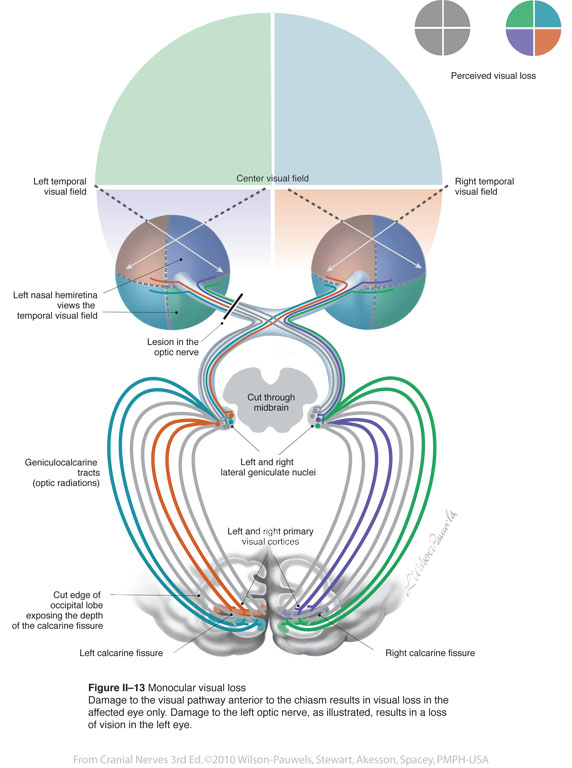 |
 |
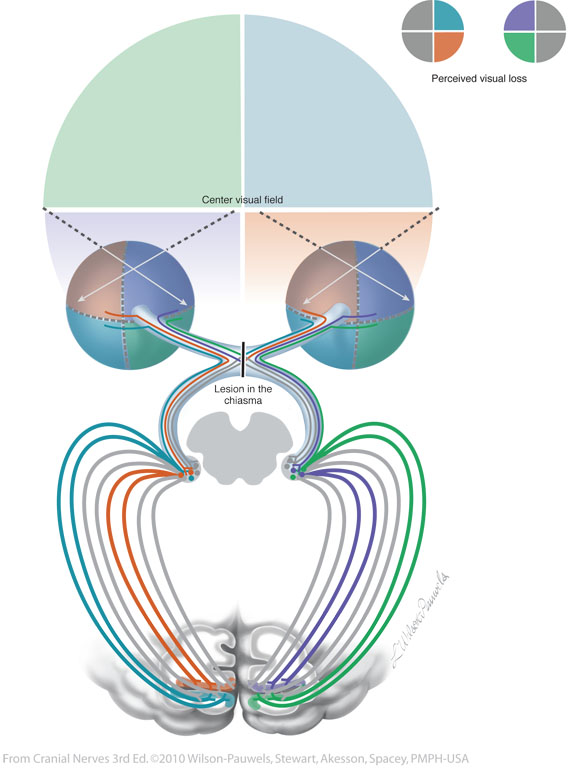
| Figure II–14 Bitemporal hemianopia. Lesions to the visual pathway at the chiasma results in visual loss in both eyes. Damage to the midline of the chiasma, as illustrated, interferes with transmission of signals from the nasal hemiretinae, which view the temporal visual fields in both eyes. | 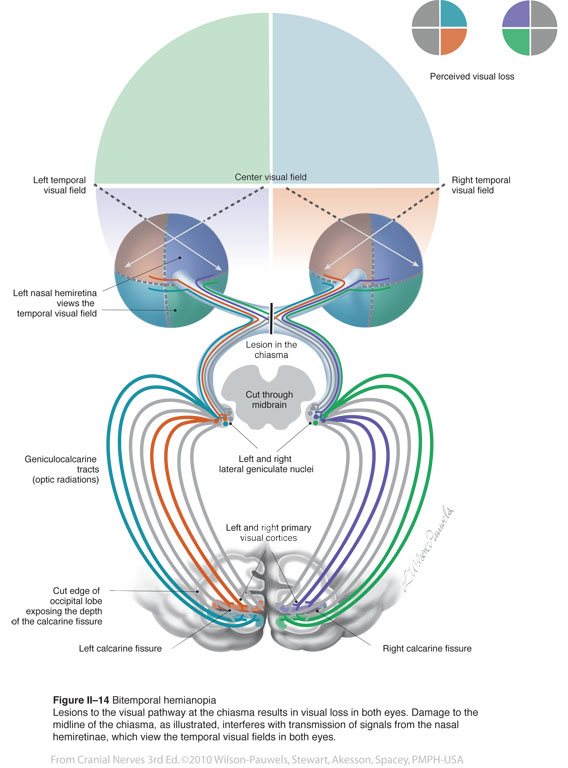 |
 |
| Figure II–15 Homonymous hemianopia. Lesions in the visual pathway posterior to the chiasma result in loss of signals from the contralateral fields in both eyes. For example, a lesion to the right optic tract, as illustrated, eliminates perception of the left visual field. |  |
 |
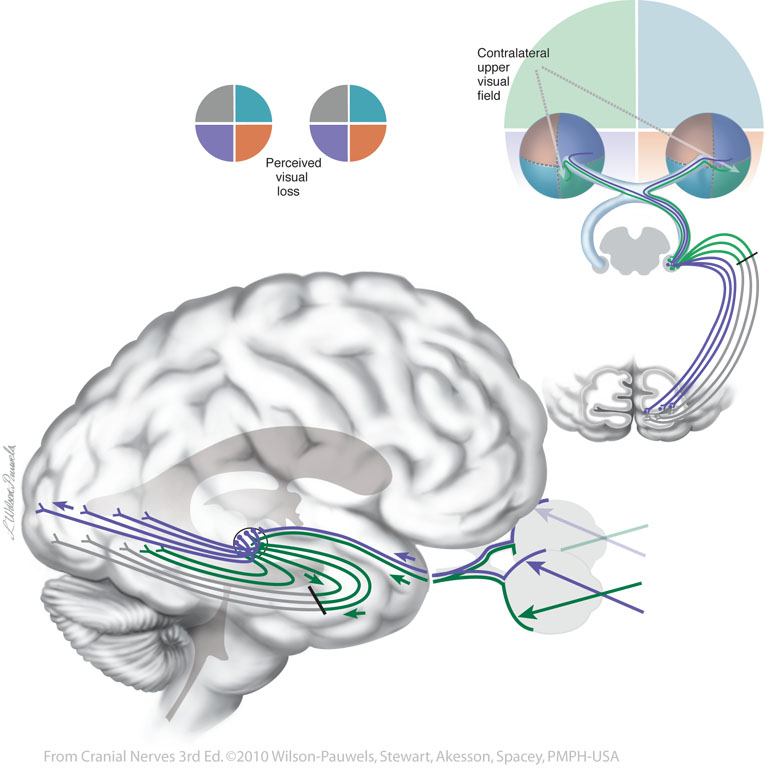
| Figure II–16 Left Upper Quadrantanopia. Lesions to the visual pathway in the right Meyer’s loop results in the loss of the contralateral upper quadrant of the visual field in both eyes. | 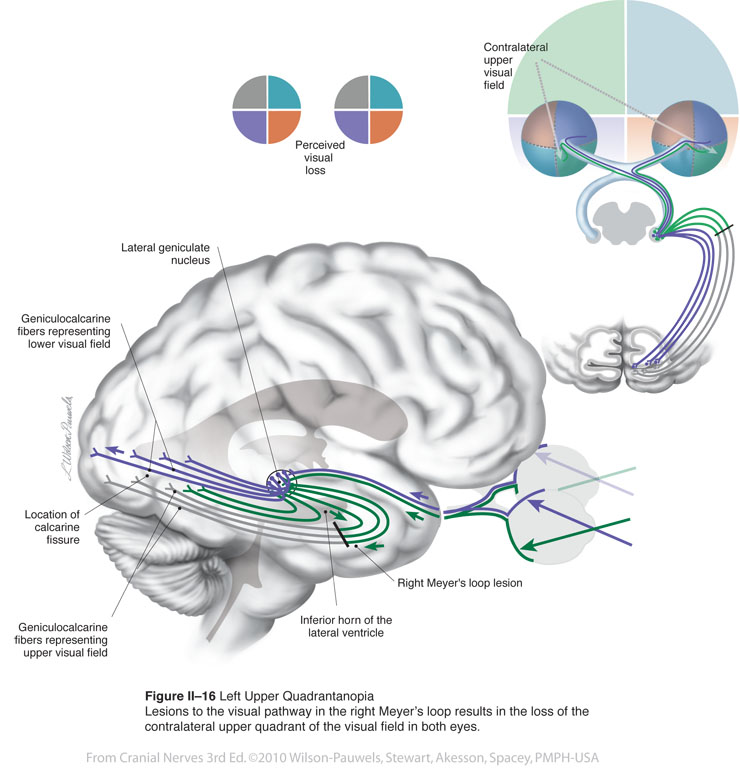 |
 |
| Figure II-17 Acuity is tested using Snellen's chart. | 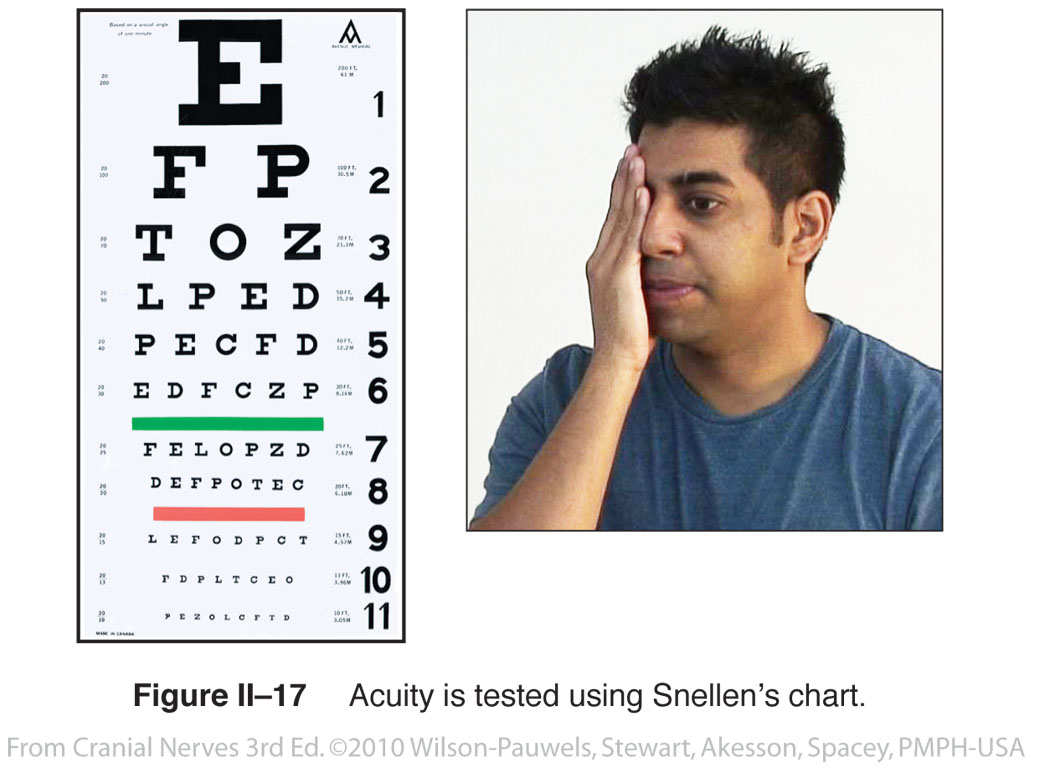 |
|
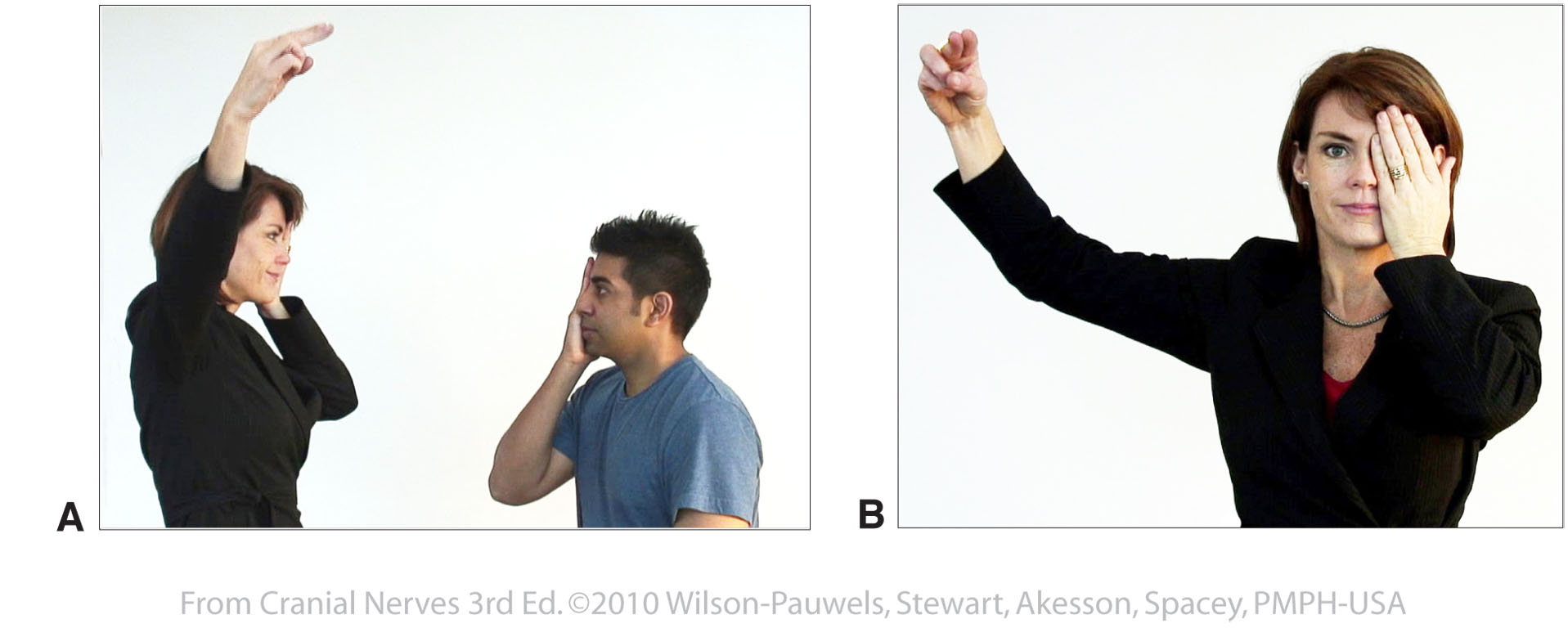
| Figure II–18 Testing of the visual field. A, Testing the upper left quadrant of the patient’s left eye (patient’s right eye and physician’s left eye are covered). B, Patient’s view of the physician testing the upper left quadrant of the patient’s left eye. | 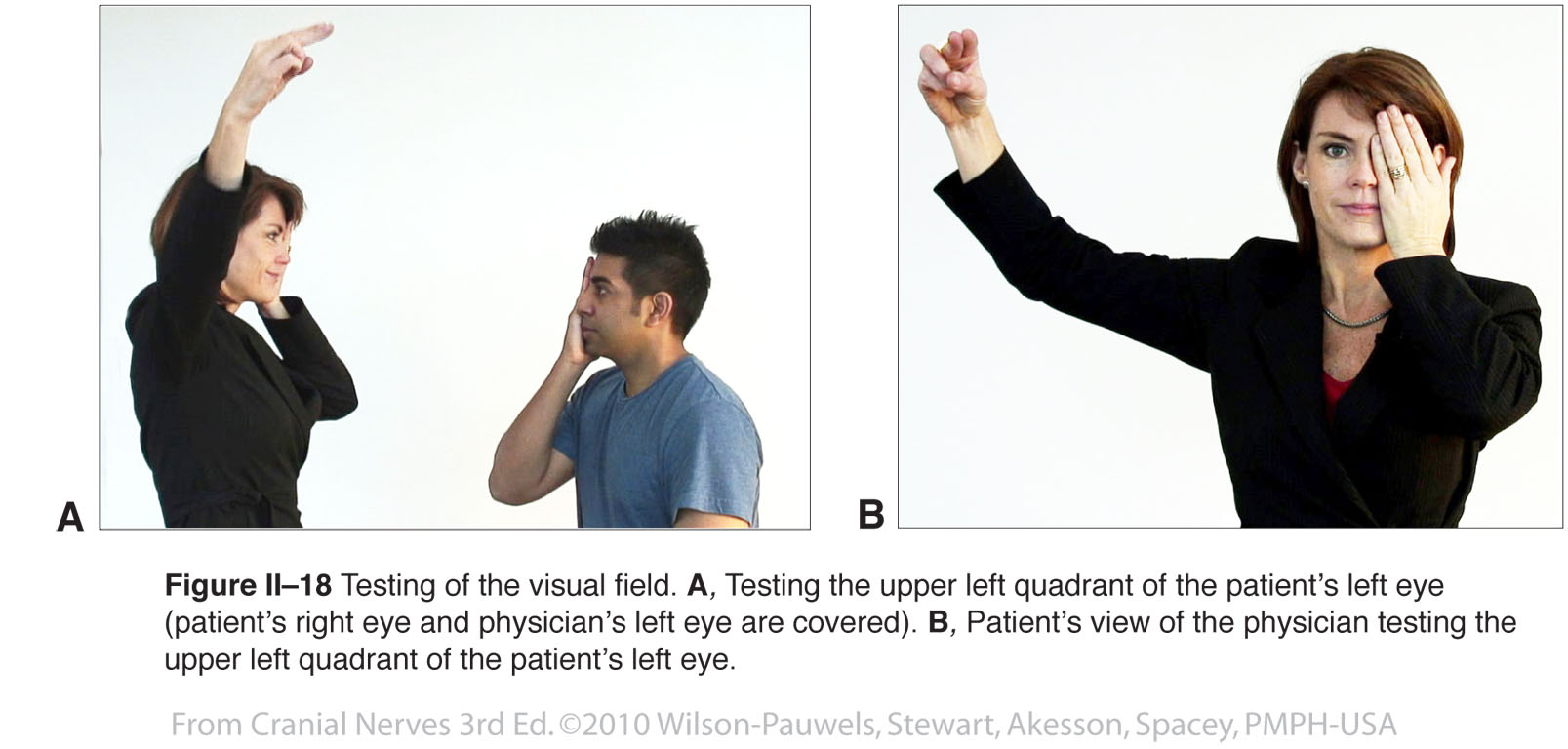 |
 |
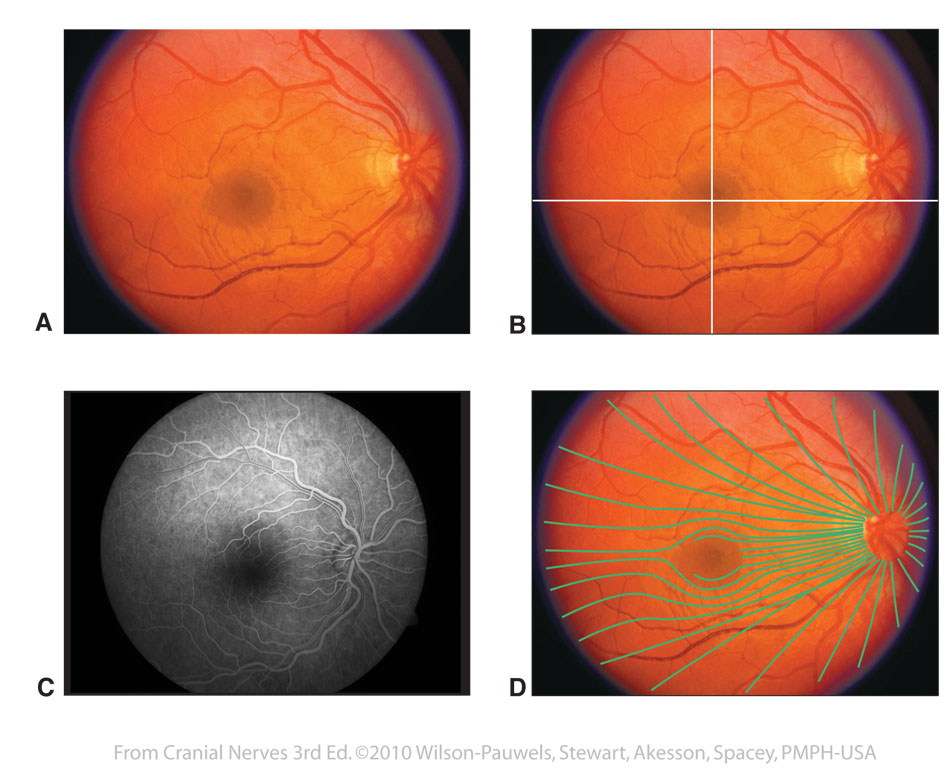
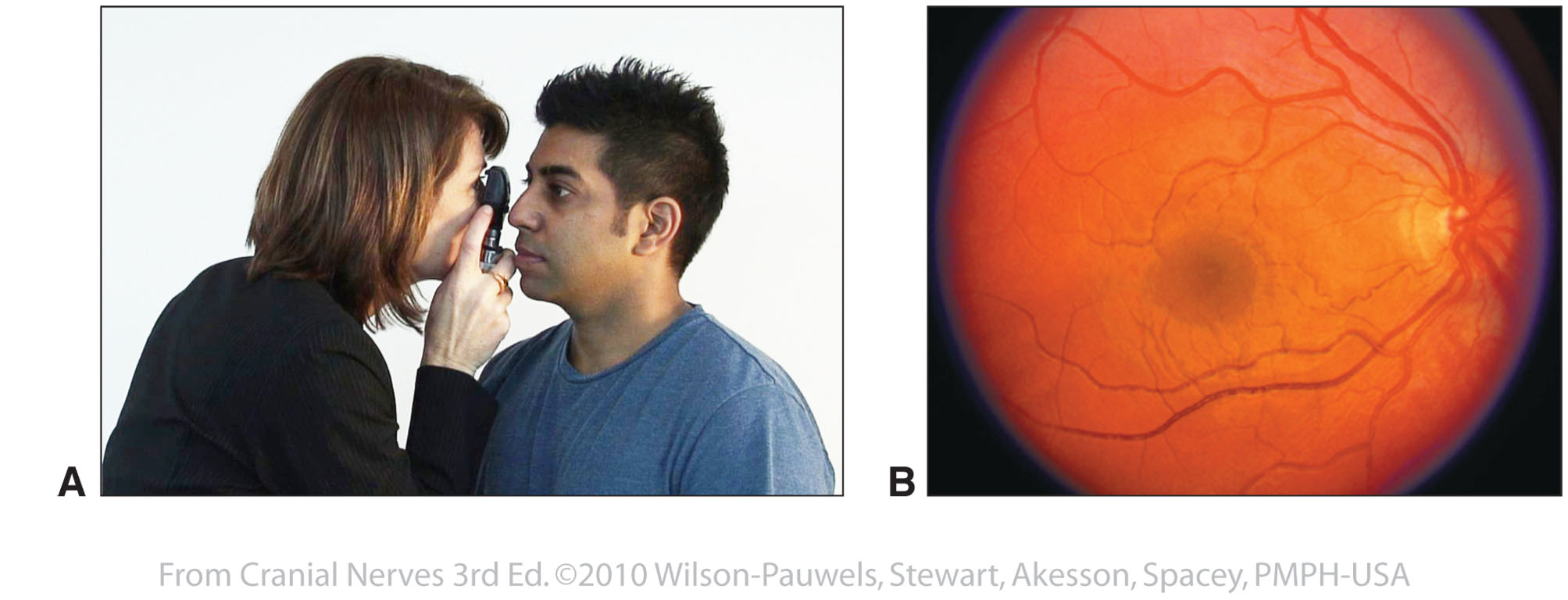
| Figure II–19 Examination of the fundus. A, The physician is examining the patient’s right fundus using an ophthalmoscope. B, Normal fundus of the right eye. (Fundus photograph courtesy of Dr. R. Buncic.) |  |
 |